盛唐环保设备
成本低,寿命长
热线电话
400-133-0799400-133-0799
400-133-0799

答:先聚丙烯(PP)吸收塔不要选择焊接工艺制造的,现在的无缝一体缠绕工艺制...
答:目前电镀废水处理常采用化学沉淀法(包括含铬废水的还原处理和含氰废水氧化...
答:废气净化塔,属于两相逆流填料塔。方法1:从下方沿切向进入塔体进气废气净...
答:工业废气指企业厂区内燃料燃烧和生产工艺过程中产生的各种排入空气的含有污...
答:废气处理设备对高浓度废气进行预处理,为防止有机废气处理系统爆炸事故,要...
Copyright© 黑豹加速器下载官网 技术支持:
电话:15879095968 杨先生 电话:400-133-0799 地址:江西省南昌市青云谱区梦想小镇2号楼305
备案号:赣ICP备18003455号-2


















 办公楼一角
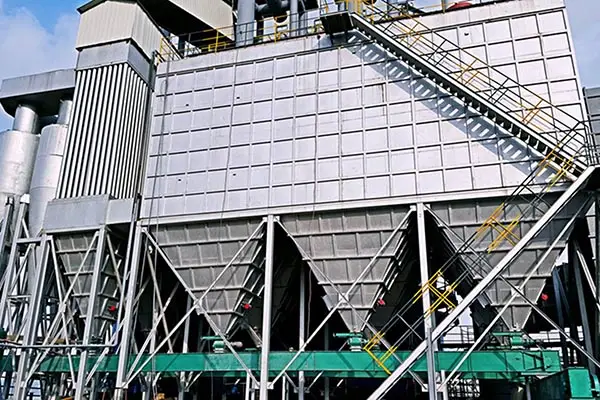
办公楼一角 高压布袋除尘器制作
高压布袋除尘器制作 车间一角
车间一角 uv光氧催化设备
uv光氧催化设备 车间一角
车间一角 车间一角
车间一角 车间一角
车间一角 UV光氧机
UV光氧机 车间一角
车间一角